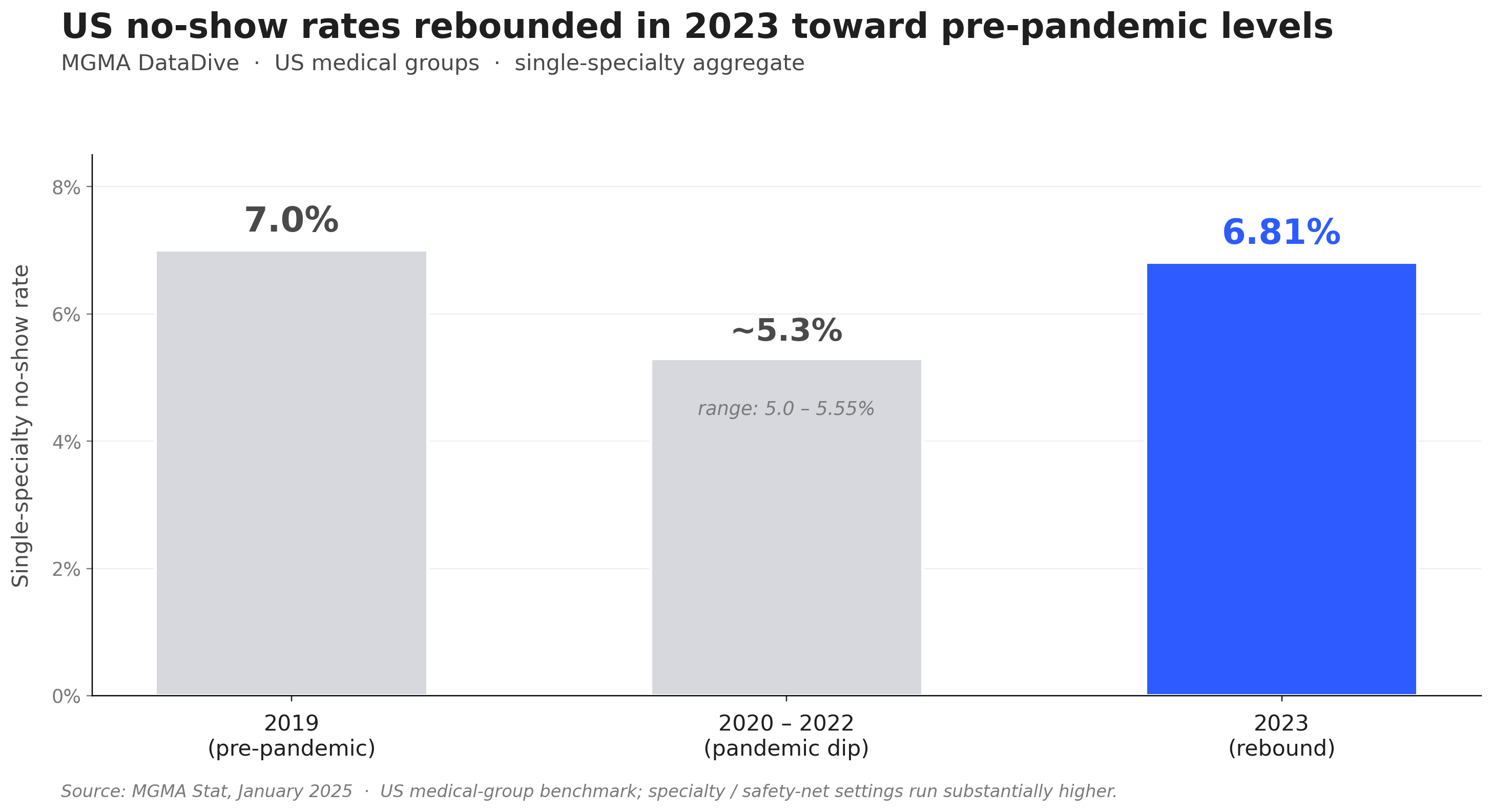
Patient no-shows are one of the most consistently documented operational problems in healthcare. In the United States, MGMA's 2025 medical-group survey reported a single-specialty aggregate no-show rate of 6.81% in 2023, up from 5–5.55% during 2020–2022 and approaching pre-pandemic levels. Specialty settings—behavioral health, hospital outpatient, safety-net clinics—run substantially higher. For individual clinics at any rate, the impact compounds: lost revenue, idle staff time, and patients whose care continuity is disrupted by appointments they never attended.
A missed appointment is not just a scheduling gap. It is a care event that did not happen—and for patients managing chronic conditions, mental health issues, or post-surgical recovery, missed appointments directly correlate with worse outcomes. In a randomized trial of 54,066 primary care patients at Kaiser Permanente Colorado, sending two reminders—one 3 days out and one 1 day out—cut missed visits to roughly 4.4%, compared to 5.3–5.8% with a single reminder (Steiner et al., 2018). SMS and phone calls performed about the same in that trial.
This article covers eight evidence-based strategies healthcare practices use to reduce no-show rates, with data on expected impact for each.
TL;DR
Strategy | Evidence Strength | Expected Impact |
Automated multi-channel reminders | ★★★★★ | ~11% attendance lift across 10 RCTs (meta-analysis) |
Reduced lead times between booking and appointment | ★★★★ | Higher attendance for short-window appointments |
Easy cancellation and rescheduling options | ★★★★ | Fewer silent no-shows |
Overbooking / double-booking for chronic no-show patients | ★★★ | Maintains slot utilization |
Telemedicine as an alternative | ★★★★ | Up to 4× lower no-show vs in-person in safety-net settings |
Patient education about consequences of missing care | ★★★ | Improves show rates for managed conditions |
Social determinants screening and navigation support | ★★★ | Reduces access-barrier no-shows |
AI-powered scheduling and communication | ★★★★ | Consistency at scale, 24/7 coverage |
The Scale of the Problem
Healthcare no-shows are expensive at every level. In the United Kingdom, NHS England estimates missed GP appointments cost the NHS approximately £216 million annually (2019 data), equivalent to over 1.2 million GP hours per year. In the United States, MGMA's 2025 survey put the 2023 single-specialty aggregate no-show rate at 6.81%—up from 5–5.55% during 2020–2022 and approaching the pre-pandemic 7% baseline.
For individual practices, the math is straightforward: a 15% no-show rate in a primary care clinic with 30 scheduled appointments per day means 4–5 unfilled slots daily. At an average revenue of 150 per visit, that is 600–750 lost per day, or approximately 150,000–$190,000 annually.
A single-site study at the Jane H. Booker Family Health Center in New Jersey (Cureus, 2026) found that coordinated operational changes—expanded laboratory hours, a centralized contact center, on-site social work and financial assistance programs—brought the average no-show rate from 18.6% in 2022 to 12.3% in 2023, a 33.8% relative reduction. As a single-site case study, the magnitude is illustrative rather than a benchmark every practice should expect.
8 Strategies to Reduce Patient No-Shows in Healthcare
1. Implement Automated Multi-Channel Appointment Reminders
The highest-impact, lowest-effort intervention available. Automated reminders sent at multiple intervals address the leading cause of healthcare no-shows (forgetfulness) and the third most common cause (lack of communication from the practice).
A 2026 meta-analysis of 10 randomized controlled trials found that appointment reminders increase attendance by roughly 11% (RR 1.11, 95% CI 1.05–1.19), with SMS (RR 1.14) and phone calls (RR 1.11) performing about equally well. For practices that already send a single reminder, the Kaiser Permanente Colorado RCT of 54,066 primary care patients cited above shows that adding a second reminder (one 3 days out, one 1 day out) lowers missed visits further—from ~5.3–5.8% to 4.4%.
Older single-site quality-improvement projects have reported much larger reductions—one breast imaging center reported a drop from 20.99% to 7.07% after introducing systematic pre-appointment phone calls (Drabkin et al., Clin Imaging 2019). Treat these as illustrative of what well-implemented reminders can achieve in a focused setting; the meta-analytic ~11% figure is the more honest expectation for a typical practice.
Recommended reminder sequence for healthcare:
- Booking confirmation: Immediately upon scheduling, including date, time, provider, location, and preparation instructions (fasting, documents to bring)
- 72 hours before: Reminder with direct link to confirm or reschedule
- 24 hours before: Final confirmation with two-way response option (Reply YES to confirm, NO to reschedule)
- 2 hours before (for same-day appointments): Last-chance confirmation
Channel hierarchy: SMS for immediacy and response, email for detail-rich communications, phone call as a fallback for patients without digital access.
2. Reduce the Lead Time Between Booking and Appointment
In a retrospective study of 120,405 appointments in Northern Italy (2022–2023), each additional day of waiting between booking and appointment was associated with a 1% increase in the odds of a no-show, with first-time visits at meaningfully higher risk than follow-ups (MDPI Healthcare, 2025). This is a single-region Italian NHS dataset—the directional relationship plausibly holds elsewhere, but the magnitude shouldn't be transplanted as-is to US practices.
A separate literature review on no-shows and service quality identifies "shortening the waiting time between scheduled and actual appointment" as one of the primary structural interventions for reducing no-shows.
Practical applications:
- Implement an open-access or advanced-access scheduling model for primary care
- Use predictive cancellation data to identify upcoming slots and pre-fill from a waitlist
- Keep some same-day or next-day slots available for acute needs, reducing the booking lag for time-sensitive patients
3. Create Easy, Low-Friction Cancellation and Rescheduling Paths
Paradoxically, making it difficult to cancel increases no-shows rather than decreasing them. When patients cannot easily reach the office to cancel, or feel uncertain about the process, they default to simply not attending.
A systematic review of non-attendance in primary care covering 26 studies (mean missed-appointment rate 15.2%) flagged unreliable reminder delivery and friction reaching the cancellation line as clinic-side contributors to no-shows. The practical implications: establish a dedicated cancellation channel, explicitly instruct patients on how to cancel in every reminder, and make self-serve cancellation available via reply-to-SMS or an online portal link.
When a patient cancels, the slot becomes available for rebooking—either through a waitlist notification or proactive outreach to patients needing follow-up visits.
4. Apply Overbooking Selectively for High-Risk Patients
Overbooking (scheduling more patients than available slots) is a standard tool in high-no-show environments. When applied to patients with documented histories of no-shows, it maintains slot utilization without forcing patients with clean attendance records into wait situations.
AAFP guidance from Family Practice Management recommends identifying chronic no-show patients in your scheduling system and either assigning them to end-of-day slots (where a missed appointment has less cascading impact) or double-booking those specific slots with the expectation that one will fill and one may not.
This approach is most appropriate for:
- Patients with three or more prior no-shows without notice
- Patients in managed care programs where no-show rates are historically elevated
- Specific appointment types (e.g., initial psychiatric evaluations) with documented high no-show rates
5. Expand Telemedicine Access
Telemedicine can dramatically reduce access-barrier no-shows—the category of missed appointments caused by transportation issues, mobility limitations, childcare conflicts, and geographic distance. A performance improvement project tracking 22,831 visits in a safety-net obstetrics clinic compared in-person and telemedicine no-show rates and found:
- In-person visit no-show rate: 35%
- Telemedicine visit no-show rate: 9%
This roughly four-fold difference persisted even in a low-income population with reduced technology access. Transportation, work schedule conflicts, and childcare were the dominant reasons for in-person no-shows—all of which telemedicine eliminates by default. The absolute numbers reflect a safety-net high-risk OB setting; the directional advantage (telemedicine substantially reduces access-barrier no-shows) is consistent across other specialty studies, but the magnitude in a general primary care setting is typically smaller.
For practices in which telemedicine is clinically appropriate, offering hybrid booking (patient's choice of in-person or video) meaningfully reduces the aggregate no-show rate.
6. Educate Patients on the Consequences of Missed Care
For patients managing chronic conditions or post-acute recovery, a missed appointment is not just a scheduling event—it is a gap in care continuity that can have clinical consequences. Communicating this explicitly can improve show rates for condition-management visits.
Effective patient education at the point of scheduling:
- Brief verbal explanation of why the upcoming appointment matters ("Your A1C follow-up helps us adjust your medication before the 90-day window closes")
- Written reminder that includes the clinical purpose, not just logistics
- For behavioral health and addiction medicine: framing the follow-up as an essential part of the treatment plan, not optional follow-through
This strategy is most effective for established patients with managed conditions. For new patients and low-urgency screenings, operational interventions (reminders, easy rescheduling) have stronger evidence bases.
7. Screen for Social Determinants of Health and Address Access Barriers
No-show data consistently shows elevated rates among patients facing access barriers: younger patients, first-visit patients, patients in lower-income areas, and patients without reliable transportation, childcare, or work flexibility. The direction here is more reliable than any specific percentage—practices serving more access-burdened populations should expect higher no-show rates and design interventions accordingly.
Targeted interventions:
- Social work or care coordinator assistance with transportation, childcare, and insurance navigation
- Sliding-scale fee availability for self-pay patients
- Financial assistance programs communicated at scheduling, not just at check-in
- Community health worker outreach for patients at highest no-show risk
The Jane H. Booker Family Health Center intervention cited earlier achieved its 33.8% no-show reduction with on-site social work and financial assistance programs as core components.
8. Use AI-Powered Scheduling and Communication Tools
Across all evidence, the consistent theme is that consistency matters: reminders only work when they are sent reliably, rescheduling paths only reduce no-shows when they are always available, and cancellation lines only prevent no-shows when someone is always on the other end. These requirements exceed what manual workflows can deliver.
Solvea provides an AI receptionist that handles inbound and outbound patient communication—confirmations, reminders, cancellation requests, rescheduling—across phone, SMS, and email, 24 hours a day. The system sends every configured reminder on schedule, handles inbound cancellation requests instantly regardless of time of day, and updates the scheduling calendar without staff intervention.
For practices where patients frequently call after hours to cancel or reschedule, an AI layer ensures these interactions are handled immediately rather than defaulting to a no-show. The patient who calls at 9 PM to say they can't make their 8 AM appointment gets an immediate response and an easy path to reschedule—instead of leaving a voicemail and feeling uncertain about whether the message was received.
Measuring Your No-Show Reduction Progress
Before and after implementing these strategies, track:
Metric | How to Measure | Target |
Overall no-show rate | No-shows ÷ total scheduled × 100 | Below 10% (primary care), below 15% (specialist) |
No-show rate by appointment type | Segment by visit type | Identify highest-risk categories |
Same-day cancellation rate | Cancellations within 24h ÷ total scheduled | Track separately from no-shows |
Slot recovery rate | Waitlist fills ÷ total cancellations | Target above 50% |
Revenue impact | No-shows per month × average visit revenue | Quantify the business case for investment |
Your AI Receptionist, Live in Minutes.
Scale your front desk with an AI that never sleeps. Solvea handles unlimited multi-channel inquiries, books appointments into your calendar automatically, and ensures zero missed opportunities around the clock.
Frequently Asked Questions
What is the average no-show rate in healthcare? It depends heavily on country, payer mix, and specialty. In the United States, MGMA's 2025 medical-group survey reported a single-specialty aggregate no-show rate of 6.81% in 2023, rebounding from 5–5.55% during 2020–2022. A separate systematic review of 26 primary care studies found a mean missed-appointment rate of 15.2% (median 12.9%). Specialty settings—behavioral health, hospital outpatient, safety-net clinics—run substantially higher and can reach 20% or more without structured interventions.
Which intervention has the strongest evidence for reducing healthcare no-shows? Automated appointment reminders. A 2026 meta-analysis of 10 RCTs found reminders lift attendance by roughly 11% (RR 1.11), with SMS and phone performing about equally well. A separate Kaiser Permanente Colorado RCT of 54,066 primary care patients found that two reminders (3 days + 1 day out) cut missed visits from 5.3–5.8% with a single reminder to 4.4%. This is also the easiest intervention to implement—it requires configuration, not ongoing labor.
What is the difference between a no-show and a late cancellation in healthcare? A no-show is when a patient does not attend and does not notify the practice. A late cancellation is a cancellation made inside the practice's defined cancellation window (commonly 24 hours). Both leave the slot unfilled, but late cancellations allow for possible rebooking through a waitlist, while no-shows do not. Track these separately to understand which problem is larger.
Can telemedicine really reduce no-shows by that much? In safety-net populations facing the heaviest access barriers, yes. A performance improvement project tracking 22,831 visits at a safety-net obstetrics clinic found in-person no-show rates of 35% versus telemedicine no-show rates of 9%—a four-fold difference that persisted even in a low-income, low-technology-access population. The magnitude varies by setting; the directional advantage (telemedicine eliminates transportation, childcare, and mobility barriers) is consistent across studies, even if the absolute numbers are smaller in a general primary care setting.
Should we charge patients for missed appointments? Healthcare no-show fees are legally and contractually complex, particularly for Medicaid and Medicare patients (federal and most state policies prohibit charging Medicaid members for missed appointments). Even where fees are permitted, the evidence base is weaker than for structural interventions (reminders, easy rescheduling, reduced lead times). Focus on reducing barriers to attendance before implementing penalties for non-attendance.
How does AI scheduling help reduce healthcare no-shows? AI tools like Solvea handle the consistency requirement that manual workflows cannot sustain: every reminder sent on schedule, every inbound cancellation handled immediately regardless of when it comes in, every rescheduling request resolved in real time. This addresses both the forgetfulness cause (reminders) and the cancellation friction cause (instant rescheduling availability) simultaneously, at the scale of any practice size.